Ophthalmic Images in Diverse Patient Populations: Difference between revisions
m (→update images) |
|||
| (48 intermediate revisions by 4 users not shown) | |||
| Line 2: | Line 2: | ||
|Authors=Ambar.Faridi | |Authors=Ambar.Faridi | ||
|Category=Articles,Miscellaneous | |Category=Articles,Miscellaneous | ||
}} | }} | ||
Currently, a disproportionate number of textbook figures and photographs are of eye conditions in white patients. Many ocular conditions can appear differently in individuals of color or those with darker skin. The purpose of this page is to share images of both common and rare pathology of the external, anterior, and posterior segments in patients of color. The American Academy of Ophthalmology's Committee for Resident Education’s DEI workgroup initiated this image collection to serve as a source for education and future versions of the [https://store.aao.org/clinical-education/product-line/bcsc-reg-basic-and-clinical-science-course.html Basic and Clinical Science Course (BCSC)] and other texts. | Currently, a disproportionate number of textbook figures and photographs are of eye conditions in white patients. Many ocular conditions can appear differently in individuals of color or those with darker skin. The purpose of this page is to share images of both common and rare pathology of the external, anterior, and posterior segments in patients of color. The American Academy of Ophthalmology's Committee for Resident Education’s DEI workgroup initiated this image collection to serve as a source for education and future versions of the [https://store.aao.org/clinical-education/product-line/bcsc-reg-basic-and-clinical-science-course.html Basic and Clinical Science Course (BCSC)] and other texts. | ||
| Line 21: | Line 20: | ||
== Amblyopia == | == Amblyopia == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File:Amblyopia.jpg|Strabismus. Strabismus is the most common underlying cause of amblyopia.With constant deviation of one eye, reduced vision occurs. Amblyopia is less likely when the deviation is intermittent or when the two eyes alternate fixation. | File:Amblyopia.jpg|Strabismus. Strabismus is the most common underlying cause of amblyopia. With constant deviation of one eye, reduced vision occurs. Amblyopia is less likely when the deviation is intermittent or when the two eyes alternate fixation. | ||
</gallery> | </gallery> | ||
| Line 42: | Line 41: | ||
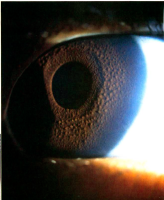
== Asteroid hyalosis == | == Asteroid hyalosis == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:AH (2).JPG|Asteroid hyalosis. Yellowish-white viterous opacities | ||
</gallery> | </gallery> | ||
== Bacterial orbital cellulitis with proptosis == | == Bacterial orbital cellulitis with proptosis == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
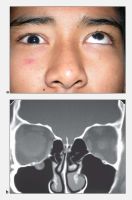
File: | File:Bacterial orbital cellulitis.png|Bacterial orbital cellulitis with proptosis (A) secondary to sinusitis (B) | ||
</gallery> | </gallery> | ||
| Line 57: | Line 56: | ||
== Basal cell carcinoma (eyelid) == | == Basal cell carcinoma (eyelid) == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:Basal Cell Carcinoma African American.png|Basal cell carcinoma | ||
</gallery> | </gallery> | ||
== Bilateral inferior oblique muscle overaction == | == Bilateral inferior oblique muscle overaction == | ||
| Line 64: | Line 63: | ||
</gallery> | </gallery> | ||
== Bilateral scleral thinning == | == Bilateral scleral thinning == | ||
<gallery widths=200 heights=200> | <gallery widths="200" heights="200"> | ||
File: | File:India patient with bilateral scleral thinning.jpg|Bilateral nonspecific orbital inflammation (orbital pseudotumor) in an 11-year old boy with a 1-week history of eye pain. Ocular rotation was markedly limited in all directions. CT confirmed proptosis and showed enlargement of all extraocular muscles. Laboratory workup was negative for thyroid disease and rheumatologic disorders. Complete resolution occurred after 1 month of corticosteroid treatment. | ||
</gallery> | </gallery> | ||
== Blepharophimosis–ptosis–epicanthus inversus syndrome == | == Blepharophimosis–ptosis–epicanthus inversus syndrome == | ||
<gallery widths=200 heights=200> | <gallery widths="200" heights="200"> | ||
File: | File:Blepharophimosis–ptosis–epicanthus inversus syndrome.jpg|Blepharophimosis–ptosis–epicanthus inversus syndrome (blepharophimosis syndrome) | ||
</gallery> | </gallery> | ||
== Blue nevi == | == Blue nevi == | ||
<gallery widths=200 heights=200> | <gallery widths="200" heights="200"> | ||
File: | File:Blue Nevi-1.jpg|Images from a 71-year-old man. A, Slit-lamp photograph showing moderately pigmented lesions in the forniceal and adjacent palpebral and bulbar conjunctiva (arrow). B, Photomicrograph revealing densely pigmented spindled melanocytes containing copious intracytoplasmic pigment, consistent with blue nevus (arrow; stain, hematoxylin–eosin; original magnification, ×200). C, Photomicrograph demonstrating removal of melanin pigment with bleach and morphologically benign dendritic cells lacking prominent nucleoli (stain, permanganate bleach; original magnification, ×200). D, Photomicrograph demonstrating SOX10 staining (arrows) within the dendritic pigmented melanocytes (stain, SOX10 immunostain with red Chromagen; original magnification, ×400) E, Photomicrograph demonstrating CD68-positive melanophages (arrow) interspersed with the dendritic melanocytes (stain, CD68 immunostain with red Chromagen; original magnification, ×400). | ||
</gallery> | </gallery> | ||
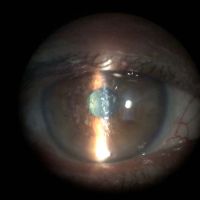
== Blue dot cataract == | == Blue dot cataract == | ||
| Line 109: | Line 107: | ||
== Choroidal metastasis == | == Choroidal metastasis == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:Asian patient with choroidal metastasis.jpg|A 65-year-old woman (patient 4) presented with choroidal metastasis (A) from breast carcinoma of 3.1-mm thickness on B-scan ultrasonography (B). After photodynamic therapy, tumor regression was seen clinically (C) and ultrasonographically (D). | ||
</gallery> | </gallery> | ||
| Line 148: | Line 146: | ||
== Conjunctival granulomas == | == Conjunctival granulomas == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:African American female patient with conjunctival granulomas.jpg|A 33-year-old woman with conjunctival granulomas. Arrow, biopsy site. The insert shows the conjunctival biopsy that revealed nonnecrotizing granuloma. | ||
</gallery> | </gallery> | ||
| Line 157: | Line 155: | ||
== Conjunctival melanoma == | == Conjunctival melanoma == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File:Photographs showing conjunctival melanoma in various races.jpg|Photographs showing conjunctival melanoma in | File:Photographs showing conjunctival melanoma in various races.jpg|Photographs showing conjunctival melanoma in patients with different skin tones. A, White man with (B) conjunctival melanoma resulting from nevus. C, African American woman with (D) conjunctival melanoma from primary acquired melanosis. E, Hispanic woman with (F) conjunctival melanoma de novo. | ||
File:Conjunctival melanoma Figure 6.png|Conjunctival melanoma of mixed pigmentation. Slit-lamp photograph of a 41-year-old man with a nodular, thickened conjunctival mass with amelanotic and melanotic areas and a prominent feeder vessel superotemporally. Systemic workup revealed distant metastases. | |||
File: | |||
</gallery> | </gallery> | ||
== Conjunctival nevus == | == Conjunctival nevus == | ||
| Line 182: | Line 178: | ||
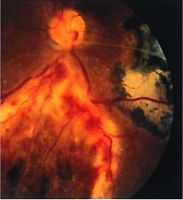
== CRAO (dark choroid) == | == CRAO (dark choroid) == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:Asian patient with central retinal artery occlusion.jpg|Fundus photograph of right eye showing severe whitening of retina and cherry-red spot at fovea (A 17-year-old woman) | ||
</gallery> | </gallery> | ||
| Line 188: | Line 184: | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File:Crawford_tube.png|A single Crawford tube is passed through both upper punctum and recovered from the right and left nares. The tube is then tied in a square knot between the nares. | File:Crawford_tube.png|A single Crawford tube is passed through both upper punctum and recovered from the right and left nares. The tube is then tied in a square knot between the nares. | ||
</gallery> | |||
== Crosslinking surgical technique == | |||
<gallery widths="200" heights="200"> | |||
File:Crosslinking_surgical_technique.jpg|Measurement of corneal pachymetry to ensure 400 μm thickness prior to UVA irradiation. | |||
</gallery> | </gallery> | ||
= D-F = | = D-F = | ||
== Dermoid cyst == | |||
<gallery widths="200" heights="200"> | |||
File:Patient_at_S%C3%A3o_Tom%C3%A9_and_Pr%C3%ADncipe_in_Africa_with_dermoid_cyst.jpg|Patient at São Tomé and Príncipe in Africa with dermoid cyst | |||
</gallery> | |||
== Descematocele == | |||
<gallery widths="200" heights="200"> | |||
File:Descematocoelee.JPG.jpg|Descematocele. Descement membrane is not disintegrated by the bacterial enzymes and so survives the destructive phase of corneal ulceration. | |||
</gallery> | |||
== Diabetic retinopathy == | == Diabetic retinopathy == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
| Line 197: | Line 206: | ||
</gallery> | </gallery> | ||
== Direct carotid–cavernous fistula (CCF) == | |||
<gallery widths="200" heights="200"> | |||
File:Direct_carotid%E2%80%93cavernous_fistula_submitted_by_e-shawn_goh_of_Singapore.jpg|Direct carotid–cavernous fistula (CCF). a. Untreated CCF with severe conjunctival chemosis and bilateral oculomotor nerve III palsy. b. Coronal CT images of the orbit demonstrate bilateral dilated superior ophthalmic veins, and enlargement of extraocular muscles. c. Coronal CT images of the cavernous sinus demonstrate convex bowing of the lateral wall. Carotid angiography provides definitive diagnosis. Doppler ultrasound may demonstrate retrograde blood flow in the superior and inferior ophthalmic veins. | |||
</gallery> | |||
== Distensible venous malformation == | |||
<gallery widths="200" heights="200"> | |||
File:Distensible_venous_malformation.jpg|Distensible venous malformation. A, Mild proptosis resulting from venous malformation of the right orbit. B, Fullness of the right superior orbit (arrow). Note the absence of dilated corkscrew conjunctival vessels. C, After Valsalva maneuver, proptosis of the right globe increases (arrow). D, T1-weighted axial MRI shows a venous malformation of the superior ophthalmic vein. | |||
</gallery> | |||
== Dystopia canthorum == | |||
<gallery widths="200" heights="200"> | |||
File:Dystopia_canthorum.jpg|Dystopia canthorum in a patient with Waardenburg syndrome. Notice that the vertical lines drawn through the puncta intersect the cornea. | |||
</gallery> | |||
== Ectopia lentis == | |||
<gallery widths="200" heights="200"> | |||
File:Patient_in_India_with_ectopia_lentis.jpg|Ectopia lentis (EL) is a major criteria for the diagnosis of Marfan syndrome, it may vary from an asymptomatic mild displacement to a significant subluxation that places the equator of the lens in the pupillary axis. Retroillumination image of ectopia lentis. | |||
</gallery> | |||
== Entrapment == | |||
<gallery widths="200" heights="200"> | |||
File:Entrapment.jpg|Orbital lymphomat. a. Right inferior rectus entrapment with inability to move the right eye upward past midline. b. Coronal CT scan demonstrating entrapment of the right inferior rectus muscle. | |||
</gallery> | |||
== Epiblepharon == | |||
<gallery widths="200" heights="200"> | |||
File:Asian_patient_with_epiblepharon.png|Epiblepharon. This condition commonly occurs in Asian patients on the lower eyelid. | |||
File:Eyelid_epiblepharon.jpg|Bilateral lower eyelid epiblepharon with persistent corneal irritation. | |||
</gallery> | |||
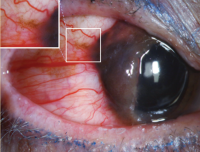
== Episcleral vessels == | == Episcleral vessels == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:Episcleral vessels.jpg|"Arterialized” episcleral vessels | ||
</gallery> | </gallery> | ||
| Line 207: | Line 242: | ||
</gallery> | </gallery> | ||
== Eyelid laceration involving the canaliculus == | |||
<gallery widths="200" heights="200"> | |||
File:Eyelid_laceration_involving_the_canaliculus.jpg|Repair of right lower eyelid laceration involving the canaliculus. A, Avulsion injury of the right lower eyelid. B, Lacrimal probe placed demonstrating the canalicular involvement. C, Lacrimal stent placement through the lacerated eyelid. D, Immediate postoperative result after reconstruction. | |||
</gallery> | |||
== Fibrous dysplasia == | |||
<gallery widths="200" heights="200"> | |||
File:Fibrous_dysplasia.jpg|Fibrous dysplasia. A, Facial asymmetry. B, CT scan shows characteristic hyperostosis of involved facial bones. | |||
</gallery> | |||
== Fish-eggs phenomenon == | |||
<gallery widths="200" heights="200"> | |||
File:Singpaore patient with fish-eggs phenomenon.jpg|Right eye fish-eggs phenomenon with multiple gas bubbles following intravitreal injection of perfluoropropane gas. | |||
</gallery> | |||
== Foveal hypoplasia == | |||
<gallery widths="200" heights="200"> | |||
File:AA0_63534.jpg|Right eye hypopigmented fundus with visible choroidal vessels and blunted foveal light reflex suggests foveal hypoplasia. | |||
</gallery> | |||
== Fuchs Uveitis Syndrome == | |||
<gallery widths="200" heights="200"> | |||
File:Fuchs Uveitis Syndrome .jpg|alt=Fuchs Uveitis Syndrome|Fuchs Uveitis Syndrome - A healthy 32-year-old woman with asymptomatic unilateral anterior uveitis, limbus-to-limbus small stellate keratic precipitates, and iris nodules and atrophy. | |||
File:Fuchs Uveitis.jpg|Fuchs Uveitis Syndrome - A 36-year-old man presented with asymptomatic uveitis in the left eye. The right eye was normal (A, C) The left eye (B, D) had 1+ cell in the anterior chamber, small stellate keratic precipitates, and mild atrophy of the iris, and a posterior subcapsular cataract. Small pupillary nodules became evident after cessation of the corticosteroid eye drops. | |||
</gallery> | |||
== Fungal ulcer == | |||
<gallery widths="200" heights="200"> | |||
File:Healed_Fungal_Ulcer_Fungal_keratitis_(1).JPG|Fungal corneal ulcers are common after vegetative ocular trauma. It can lead to a prolonged, devastating disease. | |||
</gallery> | |||
= G-I = | = G-I = | ||
== Gonococcal (neisseria) conjunctivitis == | |||
<gallery widths="200" heights="200"> | |||
File:Gonococcal_conjunctivitis.jpg|Gonococcal (Neisseria) conjunctivitis in an infant. Marked purulence is distinctive. | |||
</gallery> | |||
== Granular corneal dystrophy == | |||
<gallery widths="200" heights="200"> | |||
File:Granular_Dystrophy_(2).JPG.jpg|Characterized by Hyaline deposition in corneal stroma which stained with Mason Trichrome. | |||
File:AA0_52179.jpg|Granular corneal dystrophy. | |||
</gallery> | |||
== Gunderson conjunctival flap == | |||
<gallery widths="200" heights="200"> | |||
File:Singapore_patient_with_Gunderson_conjunctival_flap.jpg|Gunderson conjunctival flap | |||
</gallery> | |||
== Heerfordt syndrome sarcoid parotitis, lymphadenitis, and uveitis == | |||
<gallery widths="200" heights="200"> | |||
File:Heerfordt_syndrome_sarcoid_parotitis,_lymphadenitis,_and_uveitis.png|Heerfordt syndrome: sarcoid parotitis, lymphadenitis, and uveitis. This 19-year-old woman had firm, nontender glandular and lymphadenopathic edema to the left side of her face with bilateral panuveitis. | |||
</gallery> | |||
== Herpetic dendrite == | |||
<gallery widths="200" heights="200"> | |||
File:Saudi_Arabian_patient_with_herpetic_dendrite.jpg|Saudi Arabian patient with herpetic dendrite | |||
</gallery> | |||
== Skin vesicles of herpes simplex virus == | |||
<gallery widths="200" heights="200"> | |||
File:Skin_vesicles_of_herpes_simplex_virus.png|Skin vesicles of herpes simplex virus (HSV) dermatoblepharitis. | |||
</gallery> | |||
== Hurler's syndrome == | == Hurler's syndrome == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File:Aao_img_collection_hurlers_syndrome.jpg|Hurler's syndrome, cloudy corneas | File:Aao_img_collection_hurlers_syndrome.jpg|Hurler's syndrome, cloudy corneas | ||
</gallery> | </gallery> | ||
== Horner-trantas dots == | |||
<gallery widths="200" heights="200"> | |||
File:Horner-Trantas_dots.jpg|Horner-Trantas dots in vernal keratoconjunctivitis. | |||
</gallery> | |||
== Human papillomavirus (HPV) infection == | |||
<gallery widths="200" heights="200"> | |||
File:Patient_in_India_with_human_papillomavirus_(HPV)_infection.jpg|Conjunctival papillomas are associated with human papillomavirus (HPV) infection. In children, the lesions are typically manifestations of an infection acquired during delivery. In adults, conjunctival apillomas are most likely venereal and are often associated with anogenital lesions. Papillomas due to HPV more frequently rogress to malignancy in patients with the human munodeficiency virus (HIV) infection. Human papillomavirus types 6, 11, 16, and 18 have been identified in benign and malignant conjunctival lesions using various antigen and DNA detection techniques. | |||
</gallery> | |||
== Intracorneal hemorrhage == | |||
<gallery widths="200" heights="200"> | |||
File:Indian_patient_with_intracorneal_hemorrhage_.jpg|Asymptomatic, peripheral visually insignificant Intracorneal hemorrhage seen in a patient with marginal keratitis. | |||
</gallery> | |||
== Intralenticular metallic foreign body == | |||
<gallery widths="200" heights="200"> | |||
File:Patient in India with intralenticular metallic foreign body .jpg|Intralenticular metallic foreign body (IOFB) has been reported in 10% to 41% of open globe injuries. Mechanism of injury is predictive of the presence of IOFBs. High-velocity, relatively small particles are the most common foreign bodies found in the eye. Hammering, grinding, or shaving metal, machine yard work such as lawn mowing, and explosives exposure are particularly high risk. | |||
</gallery> | |||
== Iris nodular nevi == | |||
<gallery widths="200" heights="200"> | |||
File:S_diffuse_iris_nodule.png|Slit-lamp photograph of left eye of case 7 demonstrates diffuse iris nodules which are more prominent ipsilateral to her oculodermal changes. | |||
</gallery> | |||
== Iris melanoma == | == Iris melanoma == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
| Line 222: | Line 327: | ||
== Iris nevus == | == Iris nevus == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:Iris Surface Nodular nevi.jpg|Slit-lamp photograph of a 4-year old girl (case 1) shows multiple nodules distributed diffusely on the iris surface | ||
</gallery> | </gallery> | ||
= J-L = | = J-L = | ||
== Keratoglobus == | |||
<gallery widths="200" heights="200"> | |||
File:Keratoglobus.jpg|Keratoglobus. Generalized protrusion of the cornea. | |||
</gallery> | |||
== Kaposi sarcoma lesions == | |||
<gallery widths="200" heights="200"> | |||
File:Multiple_kaposi_sarcoma_lesions.jpg|(A) Multiple Kaposi sarcoma lesions on bulbar conjunctiva. (B) High-power view of one such lesion reveals its vascular nature. | |||
</gallery> | |||
== Keratopathy == | |||
<gallery widths="200" heights="200"> | |||
File:Keratopathy.jpg|Keratopathy: various degrees of severity. A, Mild keratopathy. B, Moderate keratopathy. C, Severe keratopathy. | |||
</gallery> | |||
== Keratoprosthesis surgery == | |||
<gallery widths="200" heights="200"> | |||
File:Keraprothesis_Surgery.jpg|Patient 13, a 34-year-old male who was attacked with acid. A, Preoperative state: right eye, phthisical; left eye, light perception vision. B, Post–stage 2 osteo-odonto-keratoprosthesis surgery/retinal detachment surgery, 20/150 vision. | |||
</gallery> | |||
== Laser peripheral iridotomy and anterior chamber angle == | |||
<gallery widths="200" heights="200"> | |||
File:LPI_and_anterior_chamber_angle.jpg|UBM photographs of the inferior angle of another subject before and after laser peripheral iridotomy that show flattening of the iris and the opening of the angle. | |||
</gallery> | |||
== Lateral canthotomy/cantholysis == | |||
<gallery widths="200" heights="200"> | |||
File:AA0_55157_(1).jpg|Surgical approach to the orbit combining lateral canthotomy/cantholysis, inferior transconjunctival incision, and medial Lynch (frontoethmoidal) incision. Lateral orbital rim bone removed. | |||
</gallery> | |||
== Lattice lines == | |||
<gallery widths="200" heights="200"> | |||
File:AA0_52229.jpg|Lattice lines. | |||
</gallery> | |||
== Lattice corneal dystrophy == | |||
<gallery widths="200" heights="200"> | |||
File:Patient_in_India_with_lattice_corneal_dystrophy.jpg|Lattice corneal dystrophy (LCD) is an inherited disorder of the eye characterized by the deposition of amyloid resulting in steadily progressive loss of vision. These deposits create linear, “lattice-like” opacities arising primarily in the central cornea, while the peripheral cornea is often spared. They are radially oriented and are accompanied by gradual, superficial opacification of the cornea. Recurrent epithelial erosions are often present, causing ocular irritation and additional vision loss. | |||
</gallery> | |||
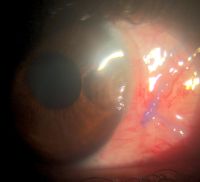
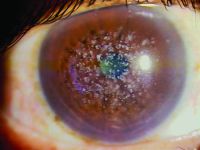
== Lens-induced glaucoma == | == Lens-induced glaucoma == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
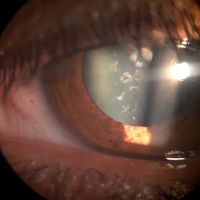
File: | File:Indian patient with lens-induced glaucoma.jpg|Lens-induced glaucoma. Patient presented with spontaneous anterior dislocated cataract which was extracted on emergency after instilling pilocarpine eye drops to prevent posterior dislocation and after one month a secondary IOL was placed with good visual recovery. | ||
</gallery> | |||
== Lens-induced phacolytic glaucoma == | |||
<gallery widths="200" heights="200"> | |||
File:AA0 54379.jpg|Cloudy cornea in adult – a masquerade of phacolytic glaucoma. A 75 year-old woman who in 1 weeks’ time had a total loss of vision, pain, redness, and total whitening of the right eye. Her vision in the right eye was PL + PR inaccurate and the left eye 6/12, N9 with glasses. Intraocular pressure was 60 in the right eye and 14 mm in the left eye. She was diagnosed as having cloudy cornea due to phacolytic glaucoma in the right eye. The patient was managed with I.v. mannitol, topical and systemic steroids, antiglaucoma medications to control IOP and reduce inflammation. After one week she underwent SICS+PCIOL implantation and she regained 6/9, N9 vision after s6 weeks postoperative | |||
</gallery> | |||
== Lentigo maligna == | |||
<gallery widths="200" heights="200"> | |||
File:Lentigo_maligna-african2.jpg|Photograph demonstrating that the involved eyelid skin displays alternating regions of hyperpigmentation and depigmentation. Eyelid margin thickening and madarosis are present. | |||
File:Lentigo_maligna-african3.jpg|Lentigo Maligna of the Eyelid. | |||
File:Lentigo_maligna-african4.jpg|Photomicrograph demonstrating polygonal dendritic melano-cytes arranged in solitary units along the basal layer of the epidermis (stain,hematoxylin– eosin; original magnification, x100). | |||
File:African_patient_with_lentigo_maligna.jpg|Photograph demonstrating a variably pigmented placoid lesion with irregular borders diffusely involving the left lower eyelid. Generalized eyelid thickening is present. | |||
</gallery> | |||
== Ocular manifestations in leukemias == | |||
<gallery widths="200" heights="200"> | |||
File:Ocular_Manifestations_in_Leukemias_in_India.png|A, Fundus photograph of a patient with acute lymphoid leukemia, showing multiple Roth spots, superficial and deep hemorrhages, and a subhyaloid bleed involving the macula. B, Fundus photograph of a patient with acute myeloid leukemia, showing dilated tortuous vessels, multiple Roth spots,and a ubhyaloid bleed in the right eye. C, Fundus photograph of a patient with chronic myeloid leukemia with bilateral disc and macular edema, cotton wool spots, Roth spots, retinal infiltrates, and neovascularization of the disc and elsewhere | |||
</gallery> | |||
== Limbal vernal keratoconjunctivitis == | |||
<gallery widths="200" heights="200"> | |||
File:Limbal_Follicle_Pseudogerontoxin.JPG|Limbal vernal keratoconjunctivitis leading to pseudogerontoxin. | |||
</gallery> | </gallery> | ||
<!--pending | <!--pending | ||
| Line 238: | Line 399: | ||
</gallery> | </gallery> | ||
--> | --> | ||
== Lymphoproliferative lesion == | |||
<gallery widths="200" heights="200"> | |||
File:Lymphoproliferative_lesion.jpg|A, Right upper eyelid ptosis and fullness with a palpable mass beneath the orbital rim. B, Coronal MRI demonstrating right lacrimal gland enlargement with infiltration of anterior orbital tissues. C, Axial MRI showing characteristic molding of the lesion to adjacent structures. D, Incisional biopsy of the abnormal infiltration of the lacrimal gland reveals orbital lymphoma (arrow). | |||
</gallery> | |||
= M-O = | = M-O = | ||
== Macular dystrophy of the retina, locus 1 == | |||
<gallery widths="200" heights="200"> | |||
File:Macular_Dystrophy_of_the_Retina,_Locus_1.jpg|Numerous yellow, drusen-like extramacular deposits were present in the retinal mid-periphery of all affected family members. | |||
</gallery> | |||
== Macular hole == | |||
<gallery widths="200" heights="200"> | |||
File:A Singapore patient with a macular hole.jpg|Color photo of macular hole | |||
</gallery> | |||
== Melanoma (conjunctiva) == | == Melanoma (conjunctiva) == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:Photographs showing conjunctival melanoma in various races.jpg|Photographs showing conjunctival melanoma in patients with various skin tones. A, White man with (B) conjunctival melanoma resulting from nevus. C, African American woman with (D) conjunctival melanoma from primary acquired melanosis. E, Hispanic woman with (F) conjunctival melanoma de novo. | ||
</gallery> | </gallery> | ||
== Metastatic carcinoma == | == Metastatic carcinoma == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
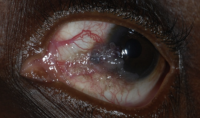
File:OM.jpg|A 37-year-old presented with ocular metastasis with primary ductal carcinoma of the left breast. | File:OM.jpg|A 37-year-old presented with ocular metastasis with primary ductal carcinoma of the left breast. She presented with complaints of redness and pain OS for 1 month, and there was a past history of a left modified radical mastectomy 3 years previously at the same institution where the patient didn’t complete the chemotherapy. On examination, OD-within normal limits, OS lids appeared edematous, circumcorneal congestion with prominent episcleral vessels seen, anterior chamber had exudative deposits and 1+ grade of cellular activity present, iris was atrophied from 3’o-5’o clock hours. | ||
</gallery> | </gallery> | ||
== Microsporidial keratoconjunctivitis == | |||
<gallery widths="200" heights="200"> | |||
File:Microsporidial_Keratoconjunctivitis-conjunctiva.png| a, Slit-lamp biomicroscopy of the conjunctiva of patient no. 6 showing diffuse conjunctival congestion with papillary changes. b, Conjunctiva of patient no. 8 shows conjunctival congestion with follicles. | |||
File:Microsporidial_Keratoconjunctivitis-scrapings.png|Pathology slide, microsporidial Keratoconjunctivitis scrapings | |||
</gallery> | |||
== Morning glory disc with exudative RD == | |||
<gallery widths="200" heights="200"> | |||
File:Singapore_patient_with_morning_Glory_Disc_with_exudative_RD.jpg|Morning glory syndrome with serous retinal detachment. Enlarged and funnel-shaped excavation of right optic disc with hyperplastic glial tissues in the central disc, peripapillary pigment abnormality, multiple anomalous straight vessels radiating circumferentially from the optic disc, inferior serous retinal detachment from 3 to 9 o'clock. | |||
</gallery> | |||
== Molluscum contagiosum == | == Molluscum contagiosum == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:Giant Eyelid Molluscum Contagiosum in a Child with AIDS.jpg|Giant eyelid molluscum contagiosum in a child with AIDS. A 6-year-old boy presented with a 3-month history of multiple, pedunculated, nodules with a central umbilication (Fig 1A). A clinical diagnosis of molluscum contagiosum was made and investigations revealed HIV infection with a CD4 count of 124/ml3. Highly active antiretroviral therapy (HAART) was initiated. The larger lesions were excised (Fig 1B). Characteristic eosinophilic intracytoplasmic inclusion bodies were seen on histopathologic examination (Fig 1C; hematoxylin-eosin 40). The child is currently on maintenance therapy with HAART with no recurrence of the lesions. | ||
File:Mollescum.jpg|Molluscum contagiosum lesions on eyelid | File:Mollescum.jpg|Molluscum contagiosum lesions on eyelid | ||
File:MG.png|Molluscum contagiosum | File:MG.png|Molluscum contagiosum | ||
</gallery> | </gallery> | ||
== Mucopolysaccharidosis == | |||
<gallery widths="200" heights="200"> | |||
File:Mucopolysaccharoidosis.JPG|Mucopolysaccharidosis. Corneal deposit disease. | |||
</gallery> | |||
== Munson sign == | |||
<gallery widths="200" heights="200"> | |||
File:Munson_sign.jpg|Munson sign. Note the angulation of the lower eyelid with the eye in downgaze. | |||
File:Munsons_Sign2.jpg|Munson's sign in keratoconus. | |||
</gallery> | |||
== Myasthenia gravis == | |||
<gallery widths="200" heights="200"> | |||
File:Myasthenia_Gravis.jpg|This 37-year-old woman with MG has pseudo–bilateral internuclear ophthalmoplegia. a. Left gaze. b. Right gaze | |||
</gallery> | |||
== Neovascular glaucoma == | == Neovascular glaucoma == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:Rubeosis (2).JPG.jpg|Rubeosis iridis | ||
</gallery> | |||
== Neurofibromatosis type I == | |||
<gallery widths="200" heights="200"> | |||
File:NF-1 pics for aao-2.jpg|Neurofibromatosis type I | |||
File:NF 1 in a child.jpg|Slit· lamp photograph of a 9-year-old boy with neurofibromatosis type I shows multiple, scattered, yellow Lisch nodules as well as more numerous brown iris nodules uniform in size and distribution. | |||
</gallery> | </gallery> | ||
== Nevus of ota (eyelids) == | == Nevus of ota (eyelids) == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
| Line 269: | Line 469: | ||
</gallery> | </gallery> | ||
== Oculodermal melanocytosis == | |||
<gallery widths="200" heights="200"> | |||
File:Iris Nodular nevi-2.jpg|Slit-lamp photograph of right eye of a 2-year-old girl (case 7) with right oculodermal melanocytosis shows multiple small nodules distributed diffusely across the iris surface. | |||
</gallery> | |||
== Ocular surface squamous neoplasia == | |||
<gallery widths="200" heights="200"> | |||
File:Indian_patient_with_ocular_surface_squamous_neoplasia.jpg|A 70-year male with very large ocular surface squamous neoplasia in right eye that was gradually increasing since 6 months. He had associated neck mass (metastasis). | |||
File:Various_grades_of_ocular_surface_squamous_neoplasia_in_East_Africa.jpg|Photographs of a pterygium and various grades of ocular surface squamous neoplasia: pterygium (A), conjunctiva intra-epithelial neoplasia (CIN) 1 (B), CIN 3 (C), carcinoma in situ (D), squamous cell carcinoma (SCC) grade 1 (E), SCC grade 2 (F), SCC grade 3 (G), and SCC with orbital invasion (H). | |||
</gallery> | |||
== Ophthalmia neonatorum == | |||
<gallery widths="200" heights="200"> | |||
File:Ophthalmia_neonatorum.jpg|Conjunctivitis presenting within 30 days of birth is diagnosed as ophthalmia neonatorum. | |||
</gallery> | |||
== Ophthalmic exam == | |||
<gallery widths="200" heights="200"> | |||
File:Ophthalmic_exam.jpg|Ophthalmic exam | |||
</gallery> | |||
== Optic disk tilting == | |||
<gallery widths="200" heights="200"> | |||
File:Chinese patient with optic disc tilting with beta peripapillary atrophy.jpg|Optic disc tilting with beta peripapillary atrophy in a 14-year-old boy with spherical equivalent refraction of −6.60 diopters and axial length of 26.30 mm. Solid arrows = edge of beta peripapillary atrophy; dotted line = axis of tilted disc. | |||
File:Optic discs with and without tilt.jpg|Optic discs with and without tilt | |||
</gallery> | |||
== Orbital floor fracture == | |||
<gallery widths="200" heights="200"> | |||
File:Orbital floor fracture.jpg|Orbital floor fracture. A, Teenaged patient following blunt trauma to the eye and orbit. Attempted gaze up and left. The left eye is unable to elevate to midline. (Note: The pupillary dilation is pharmacologic). B, Coronal CT scan of the orbit showing a small orbital floor fracture and inferior rectus muscle prolapsing into the maxillary sinus (arrow). C, Intraoperative view of a similar case showing an orbital floor defect (arrow) enlarged surgically to release and extract inferior rectus muscle. D, Two months postoperatively, the patient demonstrates resolution of upgaze limitation. | |||
</gallery> | |||
== Orbital lymphoma == | |||
<gallery widths="200" heights="200"> | |||
File:Orbital_lymphoma_submitted_by_e-shawn_goh_of_Singpore.jpg|Orbital lymphoma. a, b. Subacute onset right proptosis and upper lid mechanical ptosis with an absence of inflammatory signs. c. Coronal CT image demonstrates right lateral orbit superior and inferior infiltration by dense homogenous mass that uniformly enhances with contrast administration. Of note, the mass conforms to surrounding structures and extends along fascial planes with little surrounding inflammation. Significant disparity between tumor bulk and lack of proptosis is noted. | |||
</gallery> | |||
== Orbital myositis == | |||
<gallery widths="200" heights="200"> | |||
File:FP3005f01.png|Idiopathic orbital inflammation (orbital myositis). a. Right proptosis, lid edema and erythema, mechanical strabismus, and ptosis. b, c. Axial and coronal CT images demonstrate enlargement of all extraocular muscles in the right orbit. | |||
</gallery> | |||
== Overaction of left inferior oblique == | == Overaction of left inferior oblique == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File:Aao_img_collection_overaction_of_left_inferior_oblique.jpg| | File:Aao_img_collection_overaction_of_left_inferior_oblique.jpg|Overaction of left inferior oblique. | ||
</gallery> | </gallery> | ||
= P-R = | = P-R = | ||
| Line 279: | Line 514: | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File:Papillae_on_Tarsal_Conjunctiva.JPG.jpg|Papillary reaction of bulbar conjunctiva. Conjunctival papillae are most commonly found on bulbar conjunctiva, have a vascular core and are a sign of inflammation. | File:Papillae_on_Tarsal_Conjunctiva.JPG.jpg|Papillary reaction of bulbar conjunctiva. Conjunctival papillae are most commonly found on bulbar conjunctiva, have a vascular core and are a sign of inflammation. | ||
</gallery> | |||
== Peripheral ulcerative keratitis == | |||
<gallery widths="200" heights="200"> | |||
File:Patient_in_India_with_Peripheral_ulcerative_keratitis_.jpg|Peripheral ulcerative keratitis is a rare but potentially devastating corneal emergency. It is characterized by crescentic-shaped peripheral ulceration and may involve the sclera and conjunctiva. The etiology includes immune-mediated systemic diseases such as granulomatosis polyangiitis and rheumatoid arthritis, immune-medicated ocular diseases such as Mooren’s ulcer and non-immune mediated conditions, especially infective etiology. A host of other conditions can also mimic this entity. The patient can present in the advanced stage with corneal perforation, necessitating emergency tectonic procedures. | |||
</gallery> | |||
== Phlyctenular conjunctivitis == | |||
<gallery widths="200" heights="200"> | |||
File:Phlyctenules.jpg|Phlyctenular conjunctivitis | |||
</gallery> | |||
== Polypoidal choroidal vasculopathy (PCV) == | |||
<gallery widths="200" heights="200"> | |||
File:Polypoidal choroidal vasculopathy in white versus asian woman.png|PCV | |||
File:Polypoidal choroidopathy in african-american.jpg|PCV | |||
</gallery> | |||
== Posterior segment examination == | |||
<gallery widths="200" heights="200"> | |||
File:Posterior segment examination of hispanic.jpg|Posterior segment examination | |||
</gallery> | </gallery> | ||
== Posterior uveitis == | |||
<gallery widths="200" heights="200"> | |||
File:Posterior uveitis.jpg|A 69-year-old woman with posterior uveitis shows optic nerve head and choroidal granuloma | |||
</gallery> | |||
== Primary angle closure and OCT == | |||
<gallery widths="200" heights="200"> | |||
File:Primary_Angle_Closure_Using_OCT_in_Asians.jpg|Anterior segment optical coherence tomography image of nasal and temporal angles showing apposition between the peripheral iris and angle wall anterior to the scleral spur | |||
</gallery> | |||
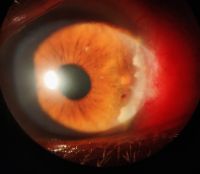
== Primary acquired melanosis (PAM) == | == Primary acquired melanosis (PAM) == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:Primary Acquired Melanoma.jpg|PAM | ||
</gallery> | </gallery> | ||
== Pterygium == | == Pterygium == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File:Indian_patient_with_asal_pterygium_with_cystic_degeneration.jpeg|A | File:Indian_patient_with_asal_pterygium_with_cystic_degeneration.jpeg|A case of inflamed nasal pterygium with cystic degeneration. ccentuates tear film abnormality causing adjacent Dellen or excavation of cornea. | ||
</gallery> | </gallery> | ||
== | == Ptosis == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File:Congenital_ptosis.jpg|Congenital ptosis | File:Congenital_ptosis.jpg|Congenital ptosis | ||
File:Measurement_of_ptosis_in_primary_gaze_with_ruler.jpg|Measurement of ptosis in primary gaze with ruler adjacent to frontal plane of face (MRD1); OD is 4 mm, OS is 1 mm. | |||
</gallery> | |||
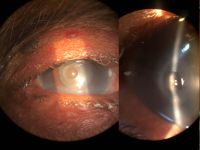
== Retinoblastoma == | |||
<gallery widths="200" heights="200"> | |||
File:African-American patient with retinoblastoma.jpg|Case 3. A 3-year-old boy with a “cloud” in this eye was found to have an iris mass with aqueous seeding (A). By clinical examination and ultrasonography (B), the posterior segment was normal. The iris tumor (A) was sampled by FNAB, demonstrating retinoblastoma. Treatment with chemotherapy and plaque radiotherapy (C) yielded complete resolution of tumor to a calcified scar (D) in the inferotemporal angle. | |||
</gallery> | |||
== Rhinosporidiosis == | |||
<gallery widths="200" heights="200"> | |||
File:AA0_62839.jpg|Fungating irregular granulation tissue in the lower tarsal conjunctiva with multiple pin head whitish lesions over its surface demonstrating underlying mature sporangia. Rhinosporidiosis is a slow-growing chronic inflammatory disorder caused by Rhinosporidiosis seeberi. It is commonly seen in groundwater, infects human beings after coming in contact with contaminated water sources. Commonly seen in nose, ears, and conjunctiva. Easily diagnosed by the typical appearance of whitish pinhead-sized lesions over the surface. Surgical excision is the only modality of management. | |||
</gallery> | </gallery> | ||
= S-Z = | = S-Z = | ||
== Salzmann’s nodular degeneration == | |||
<gallery widths="200" heights="200"> | |||
File:Patient in India with Salzmann’s nodular degeneration.jpg|Salzmann’s nodular degeneration | |||
</gallery> | |||
== Sarcoidosis == | |||
<gallery widths="200" heights="200"> | |||
File:Hispanic patient with sarcoidosis.png|Examples of biopsy-proven sarcoidosis. a. A 47-year-old woman with biopsy-proven sarcoidosis with chronic iridocyclitis. Note the large Koeppe nodules on the iris margin and gelatinous Busacca nodules (most notably in the midperipheral iris stroma at 12 o’clock). b. A 62-year-old woman with biopsy-proven pulmonary sarcoidosis and granulomatous anterior uveitis with Berlin’s nodule in the angle seen on gonioscopy. | |||
File:Sarcoidosis-02.jpg|A 34-year-old woman with bilateral lacrimal gland involvement. Arrow, biopsy site. The insert shows the lacrimal gland biopsy that revealed well-circumscribed noncaseating granulomas. | |||
File:Conjuctival granulomas.jpg|A 33-year-old woman with conjunctival granulomas. Arrow, biopsy site. The insert shows the conjunctival biopsy that revealed nonnecrotizing granuloma. | |||
</gallery> | |||
== Scleritis == | |||
<gallery widths="200" heights="200"> | |||
File:Scleritis.jpg|Diffuse anterior scleritis. Congestion involves the superficial and deep episcleral blood vessels with tortuosity, distortion, and loss of normal radial vascular pattern. | |||
</gallery> | |||
== Scleromalacia perforans == | == Scleromalacia perforans == | ||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File:Scleromalacia_Perforans_India.jpg|Scleromalacia Perforans from Long-Standing Bulbar Conjunctival Rhinosporidiosis. A 12-year-old child presented with a 6-month old painless, reddish-blue swelling superior to the upper limbus (Fig 1A). Scleral thinning with uveal show and a conjunctival mass with dot-like, yellowish-white surface excrescences were noted. Excision with a donor scleral patch graft was performed (Fig 1B). Histopathology showed partially separated squamous metaplastic epithelium(Fig 1CeD,), edematous stroma, and numerous thick walled sporangia indicating rhinosporidiosis. Several of these appeared degenerated and empty. Others showed granular debris material (Fig 1C, Hematoxylin-Eosin; Fig 1D, Gomori’s MethenamineSilver 400). Ocular rhinosporidiosis most commonly involves the tarsal conjunctiva. Scleral melt from bulbar conjunctival rhinosporidiosis is known but extremely rare. | File:Scleromalacia_Perforans_India.jpg|Scleromalacia Perforans from Long-Standing Bulbar Conjunctival Rhinosporidiosis. A 12-year-old child presented with a 6-month old painless, reddish-blue swelling superior to the upper limbus (Fig 1A). Scleral thinning with uveal show and a conjunctival mass with dot-like, yellowish-white surface excrescences were noted. Excision with a donor scleral patch graft was performed (Fig 1B). Histopathology showed partially separated squamous metaplastic epithelium(Fig 1CeD,), edematous stroma, and numerous thick walled sporangia indicating rhinosporidiosis. Several of these appeared degenerated and empty. Others showed granular debris material (Fig 1C, Hematoxylin-Eosin; Fig 1D, Gomori’s MethenamineSilver 400). Ocular rhinosporidiosis most commonly involves the tarsal conjunctiva. Scleral melt from bulbar conjunctival rhinosporidiosis is known but extremely rare. | ||
</gallery> | |||
== Shield-shaped corneal ulcers and plaques == | |||
<gallery widths="200" heights="200"> | |||
File:Shield_ulcers_and_plaque-_Bacterial_keratitis_at_the_margin_of_a_shield_ulcer.jpg|Bacterial keratitis at the margin of a shield ulcer and plaque. | |||
File:Shield_ulcers_and_plaque-lesion_grade_3_ksa.jpg|Grade 3 lesion of a patient who had simultaneous bilateral cornea plaques. Right eye with elevated yellow corneal plague that spontaneously sloughed off 1 day later. | |||
File:Shield_ulcers_and_plaque-Patient_subsequently_was_lost_to_follow-up_and_presented-KSA.jpg|Course epithelial keratopathy with roughed epithelial and fine filaments. Patient was subsequently lost to follow-up and presented 3 months later with large shield ulcer and plaque. | |||
</gallery> | |||
== Sixth nerve palsy == | |||
<gallery widths="200" heights="200"> | |||
File:Sixth_neve_palsy.png|Sixth nerve palsy. Shown here is an impairment of abduction of the right eye on right gaze. | |||
</gallery> | |||
== Spheroidal corneal degeneration == | |||
<gallery widths="200" heights="200"> | |||
File:Spheroidal_Degeneration.jpg|Known as labourer corneal degeneration, characterized by an amber-color corneal deposit or proteinaceous material. | |||
</gallery> | |||
== Squamous cell carcinoma == | |||
<gallery widths="200" heights="200"> | |||
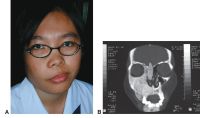
File:Squamous cell carcinoma.png|Ethmoid sinus squamous cell carcinoma. A, Photograph shows fullness of the medial canthal area overlying the mass. Axial (B) and coronal (C) | |||
File:SCC, Grade 1.jpg|Squamous cell carcinoma (SCC) grade 1 | |||
File:Conjunctival squamous cell carcinoma-01.jpg|Squamous cell tumor of conjunctiva | |||
File:Conjunctival squamous cell carcinoma-01.jpg|Conjunctival SCC with prominent leukoplakia developed in a 64-year-old man with 5 years of known HIV | |||
File:Conjunctival squamous cell carcinoma-02.jpg|Slightly pigmented conjunctival SCC developed in a 44-year-old man with 3 years of known HIV | |||
</gallery> | |||
== Staphyloma anterior == | |||
<gallery widths="200" heights="200"> | |||
File:Indian_patient_with_nixed_staphyloma_anterior.jpg|Mixed staphyloma anterior plus ciliary which is cosmetic blemish on a 4-year-old young boy. | |||
</gallery> | |||
== Stevens-Johnson Syndrome == | |||
<gallery widths="200" heights="200"> | |||
File:Stevens-Johnson_syndrome.jpg|Stevens-Johnson syndrome. | |||
File:Stevens-Johnson_syndrome-02.jpg|Patient 1, a 19-year-old male with Stevens–Johnson syndrome. A, Right eye, preoperative state, hand movements vision. B, Right eye 2 months after stage 1 surgery, healthy buccal mucosal graft. C, Right eye 26 months after stage 2 surgery, best-corrected vision of 20/20. | |||
File:SJS_1-ed.jpg|Stevens-Johnson syndrome is a type 3 hypersensitivity reaction usually related to drug exposure. | |||
</gallery> | |||
== Strabismus == | |||
<gallery widths=200 heights=200> | |||
File:AA0_2110.jpg|Incomitant strabismus. The eyes appear straight in right gaze (top) and straight-ahead gaze (middle), but a misalignment is obvious in left gaze (bottom), indicating a paralysis of the left lateral rectus muscle or a restriction of the left medial rectus. These eye positions would be found in a left sixth cranial nerve palsy | |||
</gallery> | |||
== Subfoveal choroidal thickness imaging == | |||
<gallery widths="200" heights="200"> | |||
File:Imaging subfoveal choroidal thickness images in Japan pt.jpg|OCT with choroidal thickness measurement | |||
</gallery> | |||
== Syringoma == | |||
<gallery widths=200 heights=200> | |||
File:Syringoma.jpg|Syringomas. | |||
</gallery> | |||
== Tear flow == | |||
<gallery widths=200 heights=200> | |||
File:Tear_flow.jpg|Tear flow | |||
</gallery> | |||
== Temporal hemiretinal vein occlusion == | |||
<gallery widths="200" heights="200"> | |||
File:Patient in Tunisia with temporal hemiretinal vein occlusion.jpg|CRVO/HRVO | |||
</gallery> | |||
== Tonometer == | |||
<gallery widths=200 heights=200> | |||
File:Tonometer.jpg|Tonometer | |||
</gallery> | </gallery> | ||
== | == Trachomatous trichiasis == | ||
<gallery widths="200" heights="200"> | |||
File:Patient in India with trachomatous trichiasis.png|Patient with trachomatous trichiasis | |||
File:AAX-0779.jpg|Trachomatous trichiasis (TT): at least one eyelash touching the globe. | |||
</gallery> | |||
== Tranta dots == | |||
<gallery widths="200" heights="200"> | |||
File:Tranta_Dots.JPG.jpg|Trantas dots represent collection of eosinophills in case of Limbal Vernal Keratoconjunctivitis. | |||
</gallery> | |||
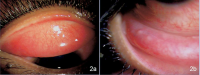
== Tuberculosis of eyelid == | |||
<gallery widths="200" heights="200"> | |||
File:Tuberculosis_of_Eyelid-India.jpg|Left lower eyelid wound with submandibular lymphadenitis. A, Patient presented with swollen, erythematous left lower eyelid with delayed eyelid wound healing after 1 week of incision and curettage. B, Fluctuant, tender submandibular swelling (arrowhead, marked) that developed within a short duration of 1 week after the first follow-up. | |||
</gallery> | |||
== Uveal melanoma == | |||
<gallery widths="200" heights="200"> | |||
File:Skin pigmentation-2.jpg|A 55-year-old man with uveal melanoma (UM) combined with oculocutaneous melanosis (OCM) who had the skin pigmentation in his right forehead, ear, cheeks, nose, eyelid, and skin folds (white arrow). B, Right eye with black conjunctival and episcleral pigmentation (white arrow). C, Fundus examination revealed a large pigmented mushroom-shaped choroidal melanoma with peripheral exudative retinal detachment (white arrow). The right fundus was dark (dark arrows) in color in comparison with the normal left eye (D). D, The normal left fundus is in orange color. | |||
</gallery> | |||
== Vernal keratoconjunctivitis == | |||
<gallery widths="200" heights="200"> | |||
File:8-year-old African-American boy with limbal vernal keratoconjunctivitis (OU) and shield ulcer plaque (OS) on slit-lamp examination.jpg|8-year-old boy with limbal vernal keratoconjunctivitis (OU) and shield ulcer plaque (OS) on slit-lamp examination | |||
File:8-year-old African-American boy with limbal vernal keratoconjunctivitis (OU) and shield ulcer plaque (OS).jpg|8-year-old boy with limbal vernal keratoconjunctivitis (OU) and shield ulcer plaque (OS) | |||
File:Patient in India with vernal keratoconjunctivitis.png|Vernal keratoconjunctivitis (VKC) is a severe disease which occurs mainly in pediatric age and is characterized by a severe and often bilateral chronic inflammation of the ocular surface. The diagnosis is generally confirmed by the finding at the ocular examination of conjunctival hyperemia, papillary hypertrophy in the tarsal conjunctiva, giant papillae and papillae in the limbus region. | |||
</gallery> | |||
== Vitiligo == | |||
<gallery widths="200" heights="200"> | |||
File:Vitiligo.jpg|Vitiligo. | |||
</gallery> | |||
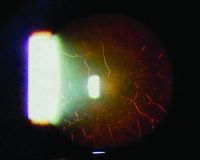
== Vitreous base avulsion == | |||
<gallery widths="200" heights="200"> | |||
File:Patient in UAE with vitreous base avulsion.png|Patient with vitreous base avulsion | |||
</gallery> | |||
== Vogt’s striae == | |||
<gallery widths="200" heights="200"> | |||
File:Patient_in_India_with_Vogt%E2%80%99s_striae.jpg|Vogt’s striae are vertical folds at the level of the posterior stroma and Descemet’s membrane , seen in patients of keratoconus. They occur in the area of maximal thinning and are best seen with a wide slit-lamp beam. These are stress lines that can be made to disappear with gentle pressure at the limbus. | |||
</gallery> | |||
== Vogt-Koyanagi-Harada (VKH) == | |||
<gallery widths="200" heights="200"> | |||
File:Chronic Vogt-Koyanagi-Harada (VKH).jpg|Chronic Vogt-Koyanagi-Harada (VKH) disease. Sunset glow fundus (A) and nummular chorioretinal scars (B) in a 54-year-old man with chronic VKH disease. Note that there is also peripapillary atrophy. Retinal pigment epithelial changes (C) are present in the fundus of a 36-year-old Hispanic woman with chronic VKH. | |||
</gallery> | |||
== West african crystalline maculopathy == | |||
<gallery widths="200" heights="200"> | |||
File:West_African_Crystalline_Maculopathy_in_a_Nigerian_Woman.jpg|West African Crystalline Maculopathy in a Nigerian Woman | |||
</gallery> | |||
== Unilateral melanocytosis == | |||
<gallery widths="200" heights="200"> | |||
File:Unilateral melanocytosis.jpg|A 58-year-old woman with diffuse unilateral melanocytosis affecting the left eye (A) and normal clinical findings in the right eye (D). B, C, Horizontal optical coherence tomography (OCT) scans through the fovea show bilaterally a normal retina with no view of the sclerochoroidal interface in the study eye (B). Magnification of OCT scans shows a thickened choroid in the study eye (E) compared with the opposite eye (F, white arrows: sclerochoroidal junction). | |||
</gallery> | |||
== Xeroderma pigmentosum == | |||
<gallery widths="200" heights="200"> | <gallery widths="200" heights="200"> | ||
File: | File:Xeroderma_Pigmentosum.jpg|Facial lentigines and ocular abnormalities in patients of different ethnicities who have xeroderma pigmentosum (XP). A, Case 1 is a 5-year-old African American XP-C patient (XP444BE) with lentigines on her skin. B, Case 2 is a 13-year-old First Nations XP-C patient (XP83BE) with many lentigines, ocular surface injection, and sunburn. C, Case 3 is a 39-year-old Hispanic XP-C patient (XP131BE) who is originally from the Dominican Republic. The patient has a history of skin cancer but no history of eyelid or ocular surface cancer. Many prominent lentigines are seen on her face and neck. The patient was fairly darkly pigmented when younger, but now pigmentation has been lost, resulting in hypopigmented areas. D, Case 4 is a 46-year-old Caucasian XP-C patient (XP1BE). 33–35 She underwent bilateral orbital exenteration at ages 32 and 36 years because of recurring invasive squamous cell carcinoma of the ocular surfaces and basal cell carcinoma of the lids, including 1 squamous cell carcinoma that occurred on the palpebral conjunctiva of the upper eyelid, a non–sun-exposed area. 36 This patient, originally light-skinned, has many darkly pigmented lentiginous areas on her face. She died of uterine cancer at age 49 years. | ||
File:Lid_and_ocular_surface_manifestations_in_patients_with_xeroderma_pigment.jpg|Lid and ocular surface manifestations in patients with xeroderma pigmentosum (XP). A, Conjunctival melanosis (arrows) in case 5, an 8-year-old Asian Indian XP-C patient (XP417BE). Note the feeder vessels to lesions (arrows). B, Early pterygium (arrowhead) and lid pigmentation (arrow) in case 2. C, Severe ectropion, entropion, and ocular inflammation in case 3. D, Lid margin keratinization (arrow) and loss of lashes in case 6, a 14-year-old patient (XP243BE). The patient has a history of skin cancer but no history of ocular surface cancer. Lentigines are present on the eyelids, and the patient has bilateral pterygium (arrowhead) and ectropion. The patient has decreased best-corrected visual acuity, possibly due to amblyopia. Localized corneal clouding at the leading edge of pterygium was suspicious for early malignancy, and biopsy was recommended. | |||
File: | |||
</gallery> | </gallery> | ||
Latest revision as of 13:05, April 3, 2024
All content on Eyewiki is protected by copyright law and the Terms of Service. This content may not be reproduced, copied, or put into any artificial intelligence program, including large language and generative AI models, without permission from the Academy.
Currently, a disproportionate number of textbook figures and photographs are of eye conditions in white patients. Many ocular conditions can appear differently in individuals of color or those with darker skin. The purpose of this page is to share images of both common and rare pathology of the external, anterior, and posterior segments in patients of color. The American Academy of Ophthalmology's Committee for Resident Education’s DEI workgroup initiated this image collection to serve as a source for education and future versions of the Basic and Clinical Science Course (BCSC) and other texts.
Visit the Academy website to learn more about its commitment to diversity, equity, and inclusion in the ophthalmic community and review educational resources related to DEI in ophthalmology.
A-C
Acanthamoeba keratitis

Classic clinical signs of Acanthamoeba keratitis. Ring-shaped infiltrate


Fundus photographs (A, C, D) and fluorescein (B) and indocyanine green (E) angiographies of typical nAMD (A, B), nnAMD (C), and PCV (D, E) in Japanese patients. nAMD neovascular AMD; nnAMD non-neovascular AMD; PCV polypoidal choroidal vasculopathy.

Amblyopia

Strabismus. Strabismus is the most common underlying cause of amblyopia. With constant deviation of one eye, reduced vision occurs. Amblyopia is less likely when the deviation is intermittent or when the two eyes alternate fixation.

Amblyogenic ptosis

Amblyogenic ptosis, left eye.

Aniridia-associated keratopathy and nystagmus

Pars Planar Tube Surgery for Aniridia-Associated Keratopathy

Pars Planar Tube Surgery for Aniridia-Associated Keratopathy


Arlt's line

Arlt’s line: a horizontal linear scar found in the watershed area between the marginal and peripheral conjunctival vasculature.

Asteroid hyalosis
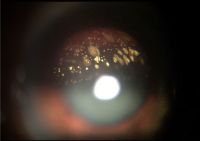
Asteroid hyalosis. Yellowish-white viterous opacities
.JPG)
Bacterial orbital cellulitis with proptosis

Bacterial orbital cellulitis with proptosis (A) secondary to sinusitis (B)

Bardet-biedl syndrome

This infant with nystagmus related to retinal dystrophy also had polydactyly (arrow), which led to the diagnosis of Bardet-Biedl syndrome. Systemic features such as renal impairment emerge in later childhood.

Basal cell carcinoma (eyelid)

Basal cell carcinoma

Bilateral inferior oblique muscle overaction

Bilateral inferior oblique muscle overaction. Overelevation in adduction, seen best in the upper fields.
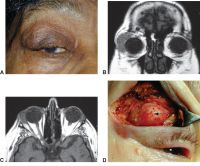
Bilateral scleral thinning

Bilateral nonspecific orbital inflammation (orbital pseudotumor) in an 11-year old boy with a 1-week history of eye pain. Ocular rotation was markedly limited in all directions. CT confirmed proptosis and showed enlargement of all extraocular muscles. Laboratory workup was negative for thyroid disease and rheumatologic disorders. Complete resolution occurred after 1 month of corticosteroid treatment.

Blepharophimosis–ptosis–epicanthus inversus syndrome

Blepharophimosis–ptosis–epicanthus inversus syndrome (blepharophimosis syndrome)

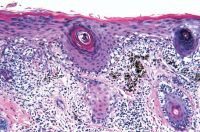
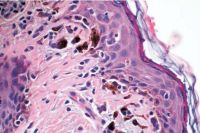
Blue nevi
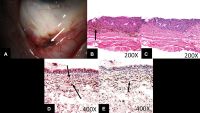
Images from a 71-year-old man. A, Slit-lamp photograph showing moderately pigmented lesions in the forniceal and adjacent palpebral and bulbar conjunctiva (arrow). B, Photomicrograph revealing densely pigmented spindled melanocytes containing copious intracytoplasmic pigment, consistent with blue nevus (arrow; stain, hematoxylin–eosin; original magnification, ×200). C, Photomicrograph demonstrating removal of melanin pigment with bleach and morphologically benign dendritic cells lacking prominent nucleoli (stain, permanganate bleach; original magnification, ×200). D, Photomicrograph demonstrating SOX10 staining (arrows) within the dendritic pigmented melanocytes (stain, SOX10 immunostain with red Chromagen; original magnification, ×400) E, Photomicrograph demonstrating CD68-positive melanophages (arrow) interspersed with the dendritic melanocytes (stain, CD68 immunostain with red Chromagen; original magnification, ×400).

Blue dot cataract
Blue dot cataract. Congenital dot-like opacities in the lens.

Blunt trauma and ruptured globe

Blunt trauma with orbital and eyelid edema

Brown syndrome

Brown syndrome. a. Child with left Brown syndrome has a hypotropia that is present with gaze up and to the right due to superior oblique restriction in the left eye. b. Eye movements and alignment are normal with gaze up and to the left.

Buphthalmos

Buphthalmos in the case of late presenting congenital glaucoma.

Carcinoma in situ
Carcinoma in situ

Cavernous hemangioma

Cavernous hemangioma. a. Normal exam and appearance. b, c. Axial MRI images demonstrate a well encapsulated, heterogeneously enhancing intraconal tumor in the right orbit. MRI findings of T1 hypointensity, and T2 hyperintensity, are useful in the differential diagnosis from neurofibroma, neurilemmoma, or hemangiopericytomas (these tumors share similar imaging characteristics on CT)

Chalazion

Chalazion.

Choroidal metastasis

A 65-year-old woman (patient 4) presented with choroidal metastasis (A) from breast carcinoma of 3.1-mm thickness on B-scan ultrasonography (B). After photodynamic therapy, tumor regression was seen clinically (C) and ultrasonographically (D).

Cicatricial trachoma

Cicatricial trachoma (TS): presence of scarring in the upper tarsal conjunctiva.

CMV retinitis
Active CMV retinitis with adjacent toxoplasmic retinochoroidal scar in Brazilian patient.

Congenital glaucoma, buphthalmos

Newborn with congenital glaucoma (right eye), buphthalmos.

Congenital coloboma

True coloboma of the upper eyelid.

Congenital lacrimal–cutaneous fistula

Congenital lacrimal–cutaneous fistula draining to the skin surface.

Congenital nevocellular nevus

Congenital nevocellular nevus of the eyelid, present since birth.

Conjunctival granulomas

A 33-year-old woman with conjunctival granulomas. Arrow, biopsy site. The insert shows the conjunctival biopsy that revealed nonnecrotizing granuloma.

Conjunctival papillomas

Conjunctival papillomas.

Conjunctival melanoma

Photographs showing conjunctival melanoma in patients with different skin tones. A, White man with (B) conjunctival melanoma resulting from nevus. C, African American woman with (D) conjunctival melanoma from primary acquired melanosis. E, Hispanic woman with (F) conjunctival melanoma de novo.
Conjunctival melanoma of mixed pigmentation. Slit-lamp photograph of a 41-year-old man with a nodular, thickened conjunctival mass with amelanotic and melanotic areas and a prominent feeder vessel superotemporally. Systemic workup revealed distant metastases.


Conjunctival nevus

Conjunctival nevi are congenital hamartomas that consist of nests of modified melanocytes (nevus cells).

Corneal arcus

Corneal arcus.

Corneal dellen
Corneal dellen. The exposed end of vicryl suture produced dellen on the adjacent portion of the cornea.

Corneal ulcer

Central bacterial corneal ulcer in a patient with severe conjunctival and corneal scarring from trachoma. Streptococcus pneumoniae was cultured.

CRAO (dark choroid)

Fundus photograph of right eye showing severe whitening of retina and cherry-red spot at fovea (A 17-year-old woman)

Crawford tube

A single Crawford tube is passed through both upper punctum and recovered from the right and left nares. The tube is then tied in a square knot between the nares.

Crosslinking surgical technique

Measurement of corneal pachymetry to ensure 400 μm thickness prior to UVA irradiation.

D-F
Dermoid cyst

Patient at São Tomé and Príncipe in Africa with dermoid cyst

Descematocele
Descematocele. Descement membrane is not disintegrated by the bacterial enzymes and so survives the destructive phase of corneal ulceration.

Diabetic retinopathy

Figure 1. Color fundus photograph of the left eye in case 1 in 1995 showing lipid exudates (arrow), cotton wool spots, and intraretinal hemorrhages of diabetic retinopathy as well as multiple refractile intraretinal crystals (arrowhead). Figure 2. Color fundus photograph of the left eye in case 1 in 2001 after focal photocoagulation for diabetic macular edema. The edema has completely resolved, and there are fewer intraretinal crystals, which are arranged in a pattern different from that in 1995. Figure 3. Color fundus photograph of the right eye in case 2 showing a frond of retinal neovascularization and many iridescent intraretinal crystals within the foveal avascular zone. Figure 4. Mid-phase fluorescein angiogram of the right eye in case 2 showing the perfused retinal neovascularization and the absence of any fluorescein angiographic sign of the crystals. Figure 5. Color fundus photograph of the right eye in case 2 one year after panretinal laser photocoagulation. Most of the crystals have resolved. Figure 6. Color fundus photograph of the right eye in case 3. The distribution of the intraretinal crystals follows the pattern of the distribution of intraretinal lipid from diabetic macular edema. The diabetic lipid exudates (arrow) can be distinguished from the refractile crystals (arrowhead).

Direct carotid–cavernous fistula (CCF)

Direct carotid–cavernous fistula (CCF). a. Untreated CCF with severe conjunctival chemosis and bilateral oculomotor nerve III palsy. b. Coronal CT images of the orbit demonstrate bilateral dilated superior ophthalmic veins, and enlargement of extraocular muscles. c. Coronal CT images of the cavernous sinus demonstrate convex bowing of the lateral wall. Carotid angiography provides definitive diagnosis. Doppler ultrasound may demonstrate retrograde blood flow in the superior and inferior ophthalmic veins.

Distensible venous malformation

Distensible venous malformation. A, Mild proptosis resulting from venous malformation of the right orbit. B, Fullness of the right superior orbit (arrow). Note the absence of dilated corkscrew conjunctival vessels. C, After Valsalva maneuver, proptosis of the right globe increases (arrow). D, T1-weighted axial MRI shows a venous malformation of the superior ophthalmic vein.

Dystopia canthorum

Dystopia canthorum in a patient with Waardenburg syndrome. Notice that the vertical lines drawn through the puncta intersect the cornea.

Ectopia lentis

Ectopia lentis (EL) is a major criteria for the diagnosis of Marfan syndrome, it may vary from an asymptomatic mild displacement to a significant subluxation that places the equator of the lens in the pupillary axis. Retroillumination image of ectopia lentis.

Entrapment
Orbital lymphomat. a. Right inferior rectus entrapment with inability to move the right eye upward past midline. b. Coronal CT scan demonstrating entrapment of the right inferior rectus muscle.

Epiblepharon

Epiblepharon. This condition commonly occurs in Asian patients on the lower eyelid.

Bilateral lower eyelid epiblepharon with persistent corneal irritation.


Episcleral vessels
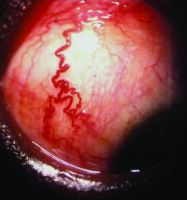
"Arterialized” episcleral vessels

Exotropia

Exotropia, left eye (child)

Eyelid laceration involving the canaliculus

Repair of right lower eyelid laceration involving the canaliculus. A, Avulsion injury of the right lower eyelid. B, Lacrimal probe placed demonstrating the canalicular involvement. C, Lacrimal stent placement through the lacerated eyelid. D, Immediate postoperative result after reconstruction.

Fibrous dysplasia
Fibrous dysplasia. A, Facial asymmetry. B, CT scan shows characteristic hyperostosis of involved facial bones.

Fish-eggs phenomenon

Right eye fish-eggs phenomenon with multiple gas bubbles following intravitreal injection of perfluoropropane gas.

Foveal hypoplasia

Right eye hypopigmented fundus with visible choroidal vessels and blunted foveal light reflex suggests foveal hypoplasia.

Fuchs Uveitis Syndrome

Fuchs Uveitis Syndrome - A healthy 32-year-old woman with asymptomatic unilateral anterior uveitis, limbus-to-limbus small stellate keratic precipitates, and iris nodules and atrophy.
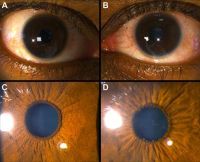
Fuchs Uveitis Syndrome - A 36-year-old man presented with asymptomatic uveitis in the left eye. The right eye was normal (A, C) The left eye (B, D) had 1+ cell in the anterior chamber, small stellate keratic precipitates, and mild atrophy of the iris, and a posterior subcapsular cataract. Small pupillary nodules became evident after cessation of the corticosteroid eye drops.


Fungal ulcer

Fungal corneal ulcers are common after vegetative ocular trauma. It can lead to a prolonged, devastating disease.
.JPG)
G-I
Gonococcal (neisseria) conjunctivitis

Gonococcal (Neisseria) conjunctivitis in an infant. Marked purulence is distinctive.

Granular corneal dystrophy
Characterized by Hyaline deposition in corneal stroma which stained with Mason Trichrome.
Granular corneal dystrophy.
.JPG.jpg)

Gunderson conjunctival flap

Gunderson conjunctival flap

Heerfordt syndrome sarcoid parotitis, lymphadenitis, and uveitis

Heerfordt syndrome: sarcoid parotitis, lymphadenitis, and uveitis. This 19-year-old woman had firm, nontender glandular and lymphadenopathic edema to the left side of her face with bilateral panuveitis.

Herpetic dendrite

Saudi Arabian patient with herpetic dendrite

Skin vesicles of herpes simplex virus

Skin vesicles of herpes simplex virus (HSV) dermatoblepharitis.

Hurler's syndrome

Hurler's syndrome, cloudy corneas

Horner-trantas dots

Horner-Trantas dots in vernal keratoconjunctivitis.

Human papillomavirus (HPV) infection

Conjunctival papillomas are associated with human papillomavirus (HPV) infection. In children, the lesions are typically manifestations of an infection acquired during delivery. In adults, conjunctival apillomas are most likely venereal and are often associated with anogenital lesions. Papillomas due to HPV more frequently rogress to malignancy in patients with the human munodeficiency virus (HIV) infection. Human papillomavirus types 6, 11, 16, and 18 have been identified in benign and malignant conjunctival lesions using various antigen and DNA detection techniques.
_infection.jpg)
Intracorneal hemorrhage

Asymptomatic, peripheral visually insignificant Intracorneal hemorrhage seen in a patient with marginal keratitis.

Intralenticular metallic foreign body

Intralenticular metallic foreign body (IOFB) has been reported in 10% to 41% of open globe injuries. Mechanism of injury is predictive of the presence of IOFBs. High-velocity, relatively small particles are the most common foreign bodies found in the eye. Hammering, grinding, or shaving metal, machine yard work such as lawn mowing, and explosives exposure are particularly high risk.

Iris nodular nevi
Slit-lamp photograph of left eye of case 7 demonstrates diffuse iris nodules which are more prominent ipsilateral to her oculodermal changes.

Iris melanoma

Iris melanoma is the most common primary neoplasm of the iris and accounts for approximately 5% of all uveal melanomas.

Iris nevus

Slit-lamp photograph of a 4-year old girl (case 1) shows multiple nodules distributed diffusely on the iris surface

J-L
Keratoglobus

Keratoglobus. Generalized protrusion of the cornea.

Kaposi sarcoma lesions

(A) Multiple Kaposi sarcoma lesions on bulbar conjunctiva. (B) High-power view of one such lesion reveals its vascular nature.

Keratopathy

Keratopathy: various degrees of severity. A, Mild keratopathy. B, Moderate keratopathy. C, Severe keratopathy.

Keratoprosthesis surgery

Patient 13, a 34-year-old male who was attacked with acid. A, Preoperative state: right eye, phthisical; left eye, light perception vision. B, Post–stage 2 osteo-odonto-keratoprosthesis surgery/retinal detachment surgery, 20/150 vision.

Laser peripheral iridotomy and anterior chamber angle

UBM photographs of the inferior angle of another subject before and after laser peripheral iridotomy that show flattening of the iris and the opening of the angle.

Lateral canthotomy/cantholysis

Surgical approach to the orbit combining lateral canthotomy/cantholysis, inferior transconjunctival incision, and medial Lynch (frontoethmoidal) incision. Lateral orbital rim bone removed.
.jpg)
Lattice lines
Lattice lines.

Lattice corneal dystrophy

Lattice corneal dystrophy (LCD) is an inherited disorder of the eye characterized by the deposition of amyloid resulting in steadily progressive loss of vision. These deposits create linear, “lattice-like” opacities arising primarily in the central cornea, while the peripheral cornea is often spared. They are radially oriented and are accompanied by gradual, superficial opacification of the cornea. Recurrent epithelial erosions are often present, causing ocular irritation and additional vision loss.

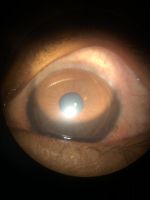
Lens-induced glaucoma

Lens-induced glaucoma. Patient presented with spontaneous anterior dislocated cataract which was extracted on emergency after instilling pilocarpine eye drops to prevent posterior dislocation and after one month a secondary IOL was placed with good visual recovery.

Lens-induced phacolytic glaucoma

Cloudy cornea in adult – a masquerade of phacolytic glaucoma. A 75 year-old woman who in 1 weeks’ time had a total loss of vision, pain, redness, and total whitening of the right eye. Her vision in the right eye was PL + PR inaccurate and the left eye 6/12, N9 with glasses. Intraocular pressure was 60 in the right eye and 14 mm in the left eye. She was diagnosed as having cloudy cornea due to phacolytic glaucoma in the right eye. The patient was managed with I.v. mannitol, topical and systemic steroids, antiglaucoma medications to control IOP and reduce inflammation. After one week she underwent SICS+PCIOL implantation and she regained 6/9, N9 vision after s6 weeks postoperative

Lentigo maligna

Photograph demonstrating that the involved eyelid skin displays alternating regions of hyperpigmentation and depigmentation. Eyelid margin thickening and madarosis are present.
Lentigo Maligna of the Eyelid.
Photomicrograph demonstrating polygonal dendritic melano-cytes arranged in solitary units along the basal layer of the epidermis (stain,hematoxylin– eosin; original magnification, x100).

Photograph demonstrating a variably pigmented placoid lesion with irregular borders diffusely involving the left lower eyelid. Generalized eyelid thickening is present.




Ocular manifestations in leukemias

A, Fundus photograph of a patient with acute lymphoid leukemia, showing multiple Roth spots, superficial and deep hemorrhages, and a subhyaloid bleed involving the macula. B, Fundus photograph of a patient with acute myeloid leukemia, showing dilated tortuous vessels, multiple Roth spots,and a ubhyaloid bleed in the right eye. C, Fundus photograph of a patient with chronic myeloid leukemia with bilateral disc and macular edema, cotton wool spots, Roth spots, retinal infiltrates, and neovascularization of the disc and elsewhere

Limbal vernal keratoconjunctivitis
Limbal vernal keratoconjunctivitis leading to pseudogerontoxin.

Lymphoproliferative lesion
A, Right upper eyelid ptosis and fullness with a palpable mass beneath the orbital rim. B, Coronal MRI demonstrating right lacrimal gland enlargement with infiltration of anterior orbital tissues. C, Axial MRI showing characteristic molding of the lesion to adjacent structures. D, Incisional biopsy of the abnormal infiltration of the lacrimal gland reveals orbital lymphoma (arrow).

M-O
Macular dystrophy of the retina, locus 1

Numerous yellow, drusen-like extramacular deposits were present in the retinal mid-periphery of all affected family members.

Macular hole

Color photo of macular hole

Melanoma (conjunctiva)
Photographs showing conjunctival melanoma in patients with various skin tones. A, White man with (B) conjunctival melanoma resulting from nevus. C, African American woman with (D) conjunctival melanoma from primary acquired melanosis. E, Hispanic woman with (F) conjunctival melanoma de novo.
Metastatic carcinoma
A 37-year-old presented with ocular metastasis with primary ductal carcinoma of the left breast. She presented with complaints of redness and pain OS for 1 month, and there was a past history of a left modified radical mastectomy 3 years previously at the same institution where the patient didn’t complete the chemotherapy. On examination, OD-within normal limits, OS lids appeared edematous, circumcorneal congestion with prominent episcleral vessels seen, anterior chamber had exudative deposits and 1+ grade of cellular activity present, iris was atrophied from 3’o-5’o clock hours.

Microsporidial keratoconjunctivitis
a, Slit-lamp biomicroscopy of the conjunctiva of patient no. 6 showing diffuse conjunctival congestion with papillary changes. b, Conjunctiva of patient no. 8 shows conjunctival congestion with follicles.

Pathology slide, microsporidial Keratoconjunctivitis scrapings


Morning glory disc with exudative RD

Morning glory syndrome with serous retinal detachment. Enlarged and funnel-shaped excavation of right optic disc with hyperplastic glial tissues in the central disc, peripapillary pigment abnormality, multiple anomalous straight vessels radiating circumferentially from the optic disc, inferior serous retinal detachment from 3 to 9 o'clock.

Molluscum contagiosum

Giant eyelid molluscum contagiosum in a child with AIDS. A 6-year-old boy presented with a 3-month history of multiple, pedunculated, nodules with a central umbilication (Fig 1A). A clinical diagnosis of molluscum contagiosum was made and investigations revealed HIV infection with a CD4 count of 124/ml3. Highly active antiretroviral therapy (HAART) was initiated. The larger lesions were excised (Fig 1B). Characteristic eosinophilic intracytoplasmic inclusion bodies were seen on histopathologic examination (Fig 1C; hematoxylin-eosin 40). The child is currently on maintenance therapy with HAART with no recurrence of the lesions.
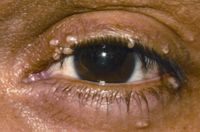
Molluscum contagiosum lesions on eyelid

Molluscum contagiosum



Mucopolysaccharidosis

Mucopolysaccharidosis. Corneal deposit disease.

Munson sign

Munson sign. Note the angulation of the lower eyelid with the eye in downgaze.

Munson's sign in keratoconus.


Myasthenia gravis
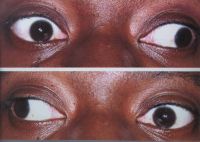
This 37-year-old woman with MG has pseudo–bilateral internuclear ophthalmoplegia. a. Left gaze. b. Right gaze

Neovascular glaucoma
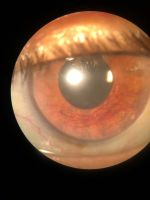
Rubeosis iridis
.JPG.jpg)
Neurofibromatosis type I

Neurofibromatosis type I

Slit· lamp photograph of a 9-year-old boy with neurofibromatosis type I shows multiple, scattered, yellow Lisch nodules as well as more numerous brown iris nodules uniform in size and distribution.


Nevus of ota (eyelids)

The slate-gray pigmentation involving the sclera and periorbital area is characteristic of oculodermal melanocytosis (nevus of Ota). Oculodermal melanocytosis is associated with an increased risk of pigmented tumors, such as choroidal melanoma.

Oculodermal melanocytosis
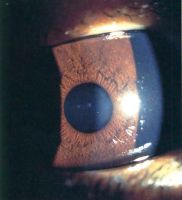
Slit-lamp photograph of right eye of a 2-year-old girl (case 7) with right oculodermal melanocytosis shows multiple small nodules distributed diffusely across the iris surface.

Ocular surface squamous neoplasia

A 70-year male with very large ocular surface squamous neoplasia in right eye that was gradually increasing since 6 months. He had associated neck mass (metastasis).

Photographs of a pterygium and various grades of ocular surface squamous neoplasia: pterygium (A), conjunctiva intra-epithelial neoplasia (CIN) 1 (B), CIN 3 (C), carcinoma in situ (D), squamous cell carcinoma (SCC) grade 1 (E), SCC grade 2 (F), SCC grade 3 (G), and SCC with orbital invasion (H).


Ophthalmia neonatorum

Conjunctivitis presenting within 30 days of birth is diagnosed as ophthalmia neonatorum.

Ophthalmic exam

Ophthalmic exam

Optic disk tilting

Optic disc tilting with beta peripapillary atrophy in a 14-year-old boy with spherical equivalent refraction of −6.60 diopters and axial length of 26.30 mm. Solid arrows = edge of beta peripapillary atrophy; dotted line = axis of tilted disc.

Optic discs with and without tilt


Orbital floor fracture

Orbital floor fracture. A, Teenaged patient following blunt trauma to the eye and orbit. Attempted gaze up and left. The left eye is unable to elevate to midline. (Note: The pupillary dilation is pharmacologic). B, Coronal CT scan of the orbit showing a small orbital floor fracture and inferior rectus muscle prolapsing into the maxillary sinus (arrow). C, Intraoperative view of a similar case showing an orbital floor defect (arrow) enlarged surgically to release and extract inferior rectus muscle. D, Two months postoperatively, the patient demonstrates resolution of upgaze limitation.

Orbital lymphoma

Orbital lymphoma. a, b. Subacute onset right proptosis and upper lid mechanical ptosis with an absence of inflammatory signs. c. Coronal CT image demonstrates right lateral orbit superior and inferior infiltration by dense homogenous mass that uniformly enhances with contrast administration. Of note, the mass conforms to surrounding structures and extends along fascial planes with little surrounding inflammation. Significant disparity between tumor bulk and lack of proptosis is noted.

Orbital myositis

Idiopathic orbital inflammation (orbital myositis). a. Right proptosis, lid edema and erythema, mechanical strabismus, and ptosis. b, c. Axial and coronal CT images demonstrate enlargement of all extraocular muscles in the right orbit.

Overaction of left inferior oblique

Overaction of left inferior oblique.

P-R
Papillary conjunctivitis
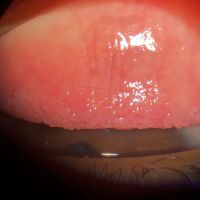
Papillary reaction of bulbar conjunctiva. Conjunctival papillae are most commonly found on bulbar conjunctiva, have a vascular core and are a sign of inflammation.

Peripheral ulcerative keratitis

Peripheral ulcerative keratitis is a rare but potentially devastating corneal emergency. It is characterized by crescentic-shaped peripheral ulceration and may involve the sclera and conjunctiva. The etiology includes immune-mediated systemic diseases such as granulomatosis polyangiitis and rheumatoid arthritis, immune-medicated ocular diseases such as Mooren’s ulcer and non-immune mediated conditions, especially infective etiology. A host of other conditions can also mimic this entity. The patient can present in the advanced stage with corneal perforation, necessitating emergency tectonic procedures.

Phlyctenular conjunctivitis

Phlyctenular conjunctivitis

Polypoidal choroidal vasculopathy (PCV)

PCV

PCV


Posterior segment examination

Posterior segment examination

Posterior uveitis

A 69-year-old woman with posterior uveitis shows optic nerve head and choroidal granuloma

Primary angle closure and OCT

Anterior segment optical coherence tomography image of nasal and temporal angles showing apposition between the peripheral iris and angle wall anterior to the scleral spur

Primary acquired melanosis (PAM)

PAM

Pterygium

A case of inflamed nasal pterygium with cystic degeneration. ccentuates tear film abnormality causing adjacent Dellen or excavation of cornea.

Ptosis

Congenital ptosis

Measurement of ptosis in primary gaze with ruler adjacent to frontal plane of face (MRD1); OD is 4 mm, OS is 1 mm.


Retinoblastoma

Case 3. A 3-year-old boy with a “cloud” in this eye was found to have an iris mass with aqueous seeding (A). By clinical examination and ultrasonography (B), the posterior segment was normal. The iris tumor (A) was sampled by FNAB, demonstrating retinoblastoma. Treatment with chemotherapy and plaque radiotherapy (C) yielded complete resolution of tumor to a calcified scar (D) in the inferotemporal angle.

Rhinosporidiosis

Fungating irregular granulation tissue in the lower tarsal conjunctiva with multiple pin head whitish lesions over its surface demonstrating underlying mature sporangia. Rhinosporidiosis is a slow-growing chronic inflammatory disorder caused by Rhinosporidiosis seeberi. It is commonly seen in groundwater, infects human beings after coming in contact with contaminated water sources. Commonly seen in nose, ears, and conjunctiva. Easily diagnosed by the typical appearance of whitish pinhead-sized lesions over the surface. Surgical excision is the only modality of management.

S-Z
Salzmann’s nodular degeneration

Salzmann’s nodular degeneration

Sarcoidosis

Examples of biopsy-proven sarcoidosis. a. A 47-year-old woman with biopsy-proven sarcoidosis with chronic iridocyclitis. Note the large Koeppe nodules on the iris margin and gelatinous Busacca nodules (most notably in the midperipheral iris stroma at 12 o’clock). b. A 62-year-old woman with biopsy-proven pulmonary sarcoidosis and granulomatous anterior uveitis with Berlin’s nodule in the angle seen on gonioscopy.
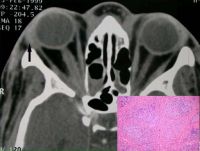
A 34-year-old woman with bilateral lacrimal gland involvement. Arrow, biopsy site. The insert shows the lacrimal gland biopsy that revealed well-circumscribed noncaseating granulomas.
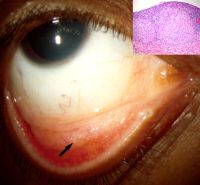
A 33-year-old woman with conjunctival granulomas. Arrow, biopsy site. The insert shows the conjunctival biopsy that revealed nonnecrotizing granuloma.



Scleritis

Diffuse anterior scleritis. Congestion involves the superficial and deep episcleral blood vessels with tortuosity, distortion, and loss of normal radial vascular pattern.

Scleromalacia perforans
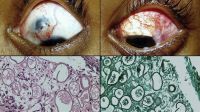
Scleromalacia Perforans from Long-Standing Bulbar Conjunctival Rhinosporidiosis. A 12-year-old child presented with a 6-month old painless, reddish-blue swelling superior to the upper limbus (Fig 1A). Scleral thinning with uveal show and a conjunctival mass with dot-like, yellowish-white surface excrescences were noted. Excision with a donor scleral patch graft was performed (Fig 1B). Histopathology showed partially separated squamous metaplastic epithelium(Fig 1CeD,), edematous stroma, and numerous thick walled sporangia indicating rhinosporidiosis. Several of these appeared degenerated and empty. Others showed granular debris material (Fig 1C, Hematoxylin-Eosin; Fig 1D, Gomori’s MethenamineSilver 400). Ocular rhinosporidiosis most commonly involves the tarsal conjunctiva. Scleral melt from bulbar conjunctival rhinosporidiosis is known but extremely rare.

Shield-shaped corneal ulcers and plaques

Bacterial keratitis at the margin of a shield ulcer and plaque.

Grade 3 lesion of a patient who had simultaneous bilateral cornea plaques. Right eye with elevated yellow corneal plague that spontaneously sloughed off 1 day later.

Course epithelial keratopathy with roughed epithelial and fine filaments. Patient was subsequently lost to follow-up and presented 3 months later with large shield ulcer and plaque.



Sixth nerve palsy

Sixth nerve palsy. Shown here is an impairment of abduction of the right eye on right gaze.

Spheroidal corneal degeneration

Known as labourer corneal degeneration, characterized by an amber-color corneal deposit or proteinaceous material.

Squamous cell carcinoma
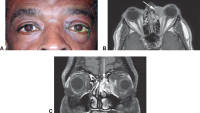
Ethmoid sinus squamous cell carcinoma. A, Photograph shows fullness of the medial canthal area overlying the mass. Axial (B) and coronal (C)
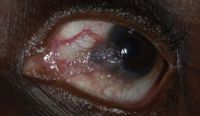
Squamous cell carcinoma (SCC) grade 1

Squamous cell tumor of conjunctiva
Conjunctival SCC with prominent leukoplakia developed in a 64-year-old man with 5 years of known HIV

Slightly pigmented conjunctival SCC developed in a 44-year-old man with 3 years of known HIV




Staphyloma anterior

Mixed staphyloma anterior plus ciliary which is cosmetic blemish on a 4-year-old young boy.

Stevens-Johnson Syndrome

Stevens-Johnson syndrome.

Patient 1, a 19-year-old male with Stevens–Johnson syndrome. A, Right eye, preoperative state, hand movements vision. B, Right eye 2 months after stage 1 surgery, healthy buccal mucosal graft. C, Right eye 26 months after stage 2 surgery, best-corrected vision of 20/20.

Stevens-Johnson syndrome is a type 3 hypersensitivity reaction usually related to drug exposure.



Strabismus

Incomitant strabismus. The eyes appear straight in right gaze (top) and straight-ahead gaze (middle), but a misalignment is obvious in left gaze (bottom), indicating a paralysis of the left lateral rectus muscle or a restriction of the left medial rectus. These eye positions would be found in a left sixth cranial nerve palsy

Subfoveal choroidal thickness imaging

OCT with choroidal thickness measurement

Syringoma

Syringomas.

Tear flow

Tear flow

Temporal hemiretinal vein occlusion

CRVO/HRVO

Tonometer

Tonometer

Trachomatous trichiasis

Patient with trachomatous trichiasis

Trachomatous trichiasis (TT): at least one eyelash touching the globe.


Tranta dots
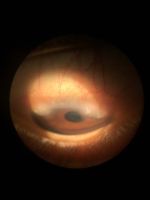
Trantas dots represent collection of eosinophills in case of Limbal Vernal Keratoconjunctivitis.

Tuberculosis of eyelid

Left lower eyelid wound with submandibular lymphadenitis. A, Patient presented with swollen, erythematous left lower eyelid with delayed eyelid wound healing after 1 week of incision and curettage. B, Fluctuant, tender submandibular swelling (arrowhead, marked) that developed within a short duration of 1 week after the first follow-up.

Uveal melanoma
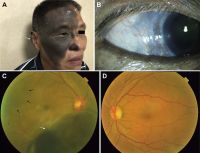
A 55-year-old man with uveal melanoma (UM) combined with oculocutaneous melanosis (OCM) who had the skin pigmentation in his right forehead, ear, cheeks, nose, eyelid, and skin folds (white arrow). B, Right eye with black conjunctival and episcleral pigmentation (white arrow). C, Fundus examination revealed a large pigmented mushroom-shaped choroidal melanoma with peripheral exudative retinal detachment (white arrow). The right fundus was dark (dark arrows) in color in comparison with the normal left eye (D). D, The normal left fundus is in orange color.

Vernal keratoconjunctivitis

8-year-old boy with limbal vernal keratoconjunctivitis (OU) and shield ulcer plaque (OS) on slit-lamp examination

8-year-old boy with limbal vernal keratoconjunctivitis (OU) and shield ulcer plaque (OS)

Vernal keratoconjunctivitis (VKC) is a severe disease which occurs mainly in pediatric age and is characterized by a severe and often bilateral chronic inflammation of the ocular surface. The diagnosis is generally confirmed by the finding at the ocular examination of conjunctival hyperemia, papillary hypertrophy in the tarsal conjunctiva, giant papillae and papillae in the limbus region.
_and_shield_ulcer_plaque_(OS)_on_slit-lamp_examination.jpg)
_and_shield_ulcer_plaque_(OS).jpg)

Vitiligo

Vitiligo.

Vitreous base avulsion

Patient with vitreous base avulsion

Vogt’s striae

Vogt’s striae are vertical folds at the level of the posterior stroma and Descemet’s membrane , seen in patients of keratoconus. They occur in the area of maximal thinning and are best seen with a wide slit-lamp beam. These are stress lines that can be made to disappear with gentle pressure at the limbus.

Vogt-Koyanagi-Harada (VKH)

Chronic Vogt-Koyanagi-Harada (VKH) disease. Sunset glow fundus (A) and nummular chorioretinal scars (B) in a 54-year-old man with chronic VKH disease. Note that there is also peripapillary atrophy. Retinal pigment epithelial changes (C) are present in the fundus of a 36-year-old Hispanic woman with chronic VKH.
.jpg)
West african crystalline maculopathy

West African Crystalline Maculopathy in a Nigerian Woman

Unilateral melanocytosis
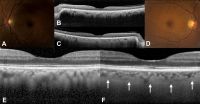
A 58-year-old woman with diffuse unilateral melanocytosis affecting the left eye (A) and normal clinical findings in the right eye (D). B, C, Horizontal optical coherence tomography (OCT) scans through the fovea show bilaterally a normal retina with no view of the sclerochoroidal interface in the study eye (B). Magnification of OCT scans shows a thickened choroid in the study eye (E) compared with the opposite eye (F, white arrows: sclerochoroidal junction).

Xeroderma pigmentosum

Facial lentigines and ocular abnormalities in patients of different ethnicities who have xeroderma pigmentosum (XP). A, Case 1 is a 5-year-old African American XP-C patient (XP444BE) with lentigines on her skin. B, Case 2 is a 13-year-old First Nations XP-C patient (XP83BE) with many lentigines, ocular surface injection, and sunburn. C, Case 3 is a 39-year-old Hispanic XP-C patient (XP131BE) who is originally from the Dominican Republic. The patient has a history of skin cancer but no history of eyelid or ocular surface cancer. Many prominent lentigines are seen on her face and neck. The patient was fairly darkly pigmented when younger, but now pigmentation has been lost, resulting in hypopigmented areas. D, Case 4 is a 46-year-old Caucasian XP-C patient (XP1BE). 33–35 She underwent bilateral orbital exenteration at ages 32 and 36 years because of recurring invasive squamous cell carcinoma of the ocular surfaces and basal cell carcinoma of the lids, including 1 squamous cell carcinoma that occurred on the palpebral conjunctiva of the upper eyelid, a non–sun-exposed area. 36 This patient, originally light-skinned, has many darkly pigmented lentiginous areas on her face. She died of uterine cancer at age 49 years.

Lid and ocular surface manifestations in patients with xeroderma pigmentosum (XP). A, Conjunctival melanosis (arrows) in case 5, an 8-year-old Asian Indian XP-C patient (XP417BE). Note the feeder vessels to lesions (arrows). B, Early pterygium (arrowhead) and lid pigmentation (arrow) in case 2. C, Severe ectropion, entropion, and ocular inflammation in case 3. D, Lid margin keratinization (arrow) and loss of lashes in case 6, a 14-year-old patient (XP243BE). The patient has a history of skin cancer but no history of ocular surface cancer. Lentigines are present on the eyelids, and the patient has bilateral pterygium (arrowhead) and ectropion. The patient has decreased best-corrected visual acuity, possibly due to amblyopia. Localized corneal clouding at the leading edge of pterygium was suspicious for early malignancy, and biopsy was recommended.

